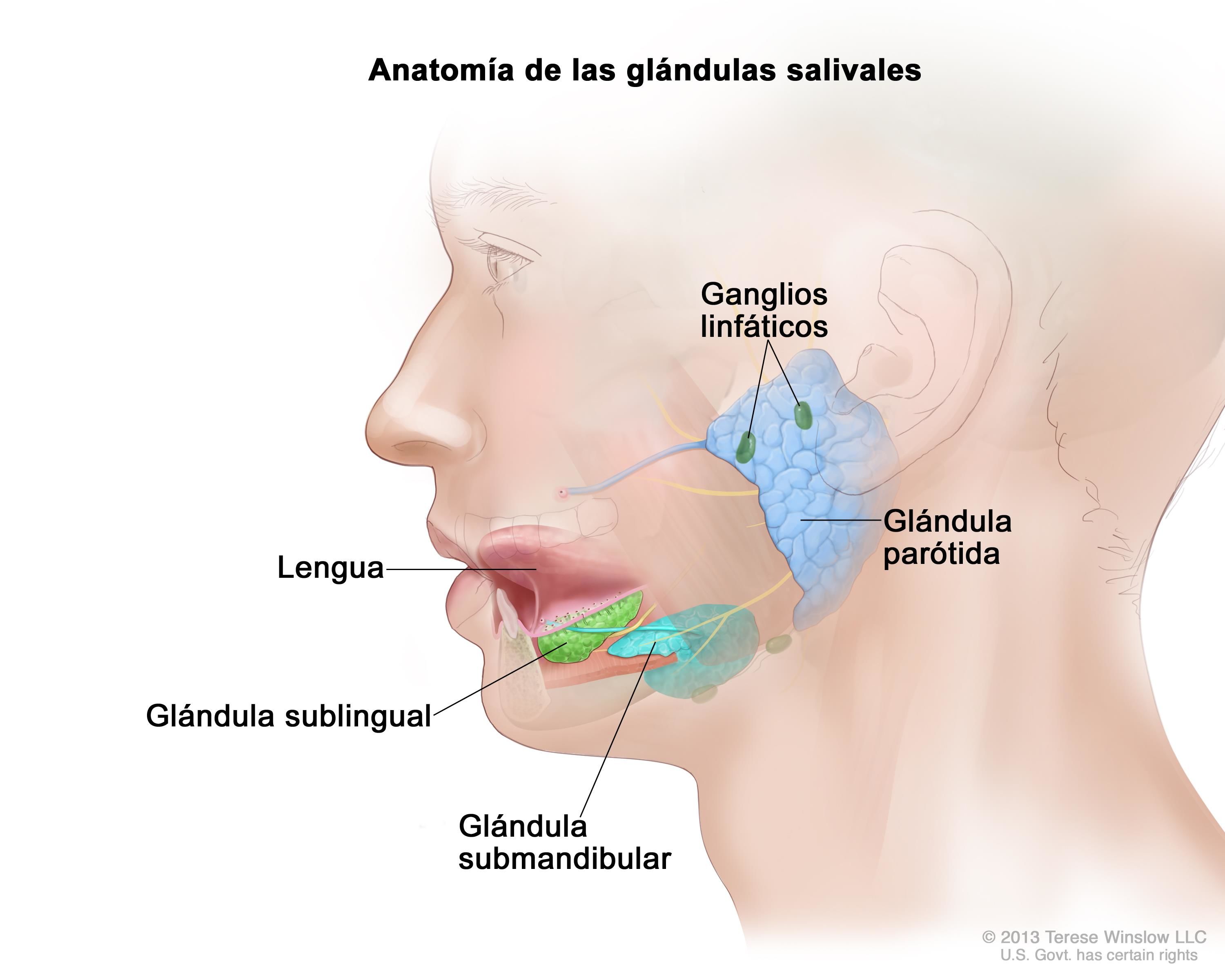
The salivary glands produce saliva and are necessary for maintaining a sufficient level of moisture in the mouth. There are 3 major salivary glands (parotid, submaxillary and sublingual) which are found on each side of the face and mouth. There are also one thousand minor salivary glands inside the mouth.
Salivary glands
What are the salivary glands?
Tumours in the salivary glands
Most tumours (80%) originate in the parotid gland, with 15% originating in the submaxillary gland. Most of these tumours are benign.
In all cases, the initial symptom is the appearance of a “lump” or swelling in the salivary glands. For this reason, an appointment with an ENT specialist (otolaryngologist) is necessary if you find a “lump” on the cheek, in front of the ear, in the mouth or on the neck, and also you feel any pain when eating or chewing.
How are the tumours diagnosed?
The ENT specialist will carry out a full manual examination for lumps on the salivary glands before following up with a completely painless fine-needle aspiration (FNA) procedure, to extract the cells for analysis.
Radiological screening (CAT, MRI scan), and if required, a biopsy.
What are the different types of salivary gland tumours?
- Benign: the most common benign tumours (70%) are what we call a mixed tumour or pleomorphic adenoma, almost always found in the parotid gland. If it is not removed, it can turn into a malignant tumour. Other benign tumours, which are far less common, include Warthin and adenoma tumours. All of these types of tumour are slow growing;
- Malignant: the most common malignant tumours are carcinomas (mucoepidermoid carcinoma, adenocarcinoma and adenoid cystic carcinoma). Fortunately, they only represent 15% of all tumours found in the salivary gland. In addition to swelling and/or lumps, they can cause facial pain and paralysis.
How are they treated?
For benign salivary gland tumours, the treatment will always be the removal of the tumour.
For malignant salivary gland tumours, the affected salivary gland and the lymph nodes of the surrounding areas of the neck will be removed. Furthermore, depending on the type and extent of the tumour, radiotherapy and, in exceptional cases, chemotherapy may be required to complete the treatment.
The surgical removal of the parotid gland will leave a recess or depression in the cheek.
We use a variety of techniques to eliminate any undesired after-effects:
- refilling the affected areas with collagen to prevent facial depression
- “Lifting” procedure (as used by plastic surgeons) to prevent visible scarring
- electrophysiological monitoring to prevent damage to the facial nerves
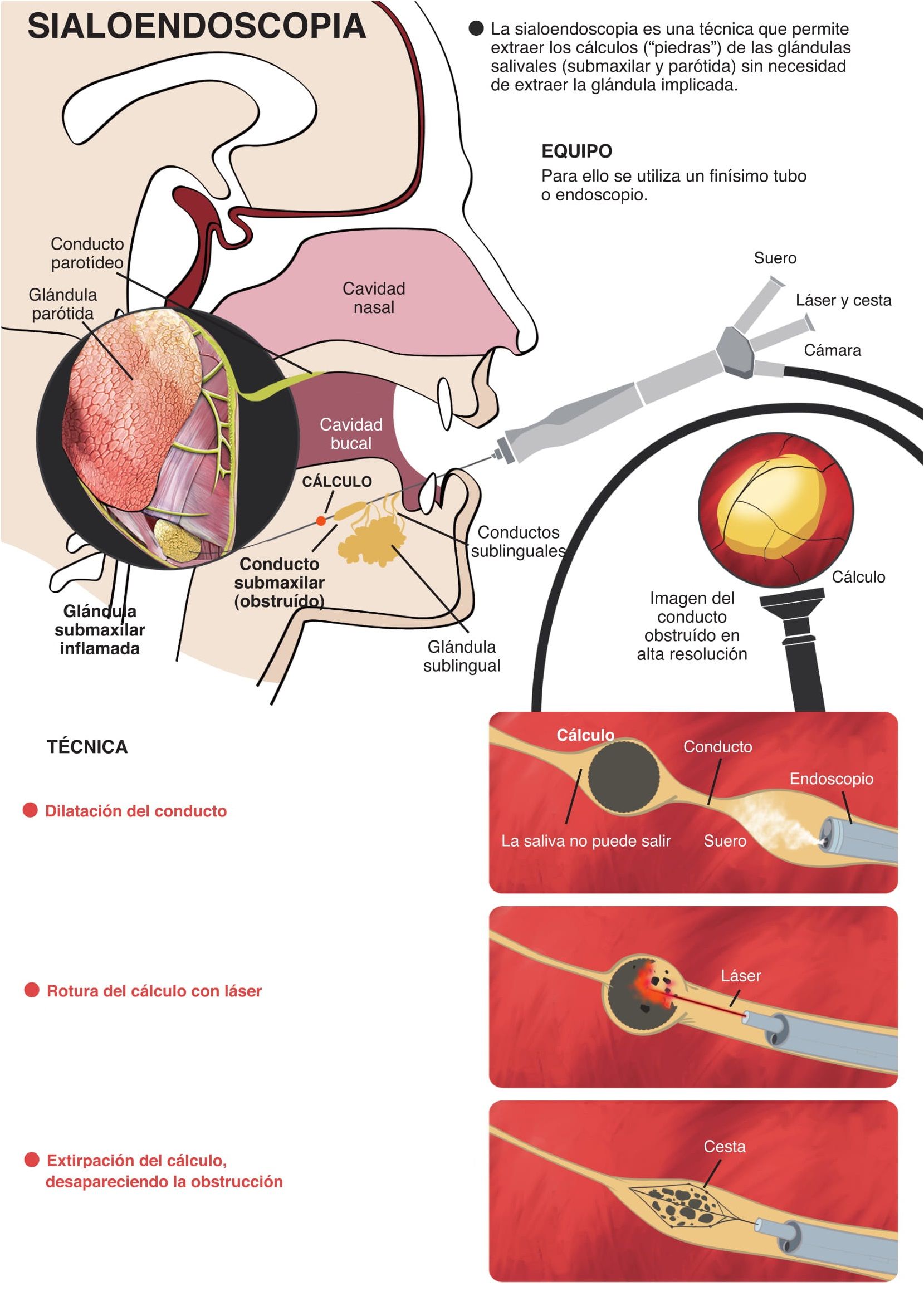
SIALOENDOSCOPIA
Se trata de una técnica que permite un tratamiento mínimamente invasivo de muchos de los problemas que afectan a las glándulas salivales, tanto las glándulas submaxilares como las glándulas parótidas, las cuales fabrican la saliva y la vierten en el interior de la boca.
Hay diferentes enfermedades que afectan a estas glándulas, especialmente la sialolitiasis, es decir la presencia de cálculos que obstruyen la glándula, impidiendo la eliminación de la saliva y provocando cólicos, inflamaciones y/o infecciones.
Hasta ahora el tratamiento de cálculos (o “piedras”) consistía en la extirpación de la glándula afectada, con la consiguiente cicatriz, el riesgo de lesionar el llamado nervio marginal, un postoperatorio doloroso, etc.
Gracias a una nueva técnica, la sialoendoscopia (endoscopia de las glándulas salivales), se puede extraer el cálculo sin necesidad de extraer la glándula afectada.
Para ello se introducen los endoscopios (pequeños tubos de 1,1mm de diámetro) en la glándula, a través de los cuales se extirpará el cálculo.
Esta técnica presenta una serie de importantes ventajas en relación a la cirugía clásica, como son: disminución del tiempo operatorio y de ingreso, anestesia mucho más ligera, ausencia de daños estéticos (entre ellos la cicatriz), menores molestias postoperatorias, conservación de la parte sana de la glándula, y rápida recuperación del paciente.

