Electronystagmography
IMBALANCE OR INSECURITY WHILE WALKING ARE SYMPTOMS OF VERTIGO








Fig. 9

Fig. 10

España aprieta los dientes. (El País 06/08/2014)
VERTIGO UNIT
What is vertigo?
Vertigo, or dizziness, is a spinning sensation where the individual feels as if they or the objects around them are moving. This sensation is almost always accompanied by unsteadiness or impaired balance and in some cases by symptoms such as nausea, sweating, vomiting, etc. Sometimes the patient will only experience unsteadiness or impaired balance when walking.
Anybody can suffer from vertigo; the symptoms can develop in children, young adults and the elderly alike.
Often with children, problems of the middle ear are brought to light through vertigo; in the elderly, cases of vertigo and dizziness can develop into chronic instability.
What causes vertigo?
The main causes of vertigo or dizziness are changes to the ear. In order of frequency, the causes include benign paroxysmal positional vertigo (BPPV), Ménière’s disease, and vestibular neuronitis, which are the reasons behind approximately fifty per cent of consultations for vertigo and dizziness.
Other changes to the ear include tumours (acoustic neuroma or vestibular schwannoma), traumas, infections, toxic substances (drugs that damage the ear) or idiopathic reactions, which represent 33% of all cases of vertigo.
Causes can also be neurological: in order of frequency, vascular causes, cervical alterations and multiple sclerosis (MS).
Ménière’s disease
Ménière’s disease is one of the most common types of vertigo. The disorder is characterised by episodes of vertigo, accompanied by nausea, vomiting and sweating, and progressive hearing impairment and tinnitus (noises in the ear).
If the initial treatment (medication) fails, which is often the case, we will resort to intratympanic gentamicin treatment. Under local anaesthetic, at our clinic we will inject a sufficient quantity of the drug (gentamicin) directly into the ear for it to have the desired effect.
Intratympanic gentamicin injections are the most modern and effective treatment available. After receiving the injections, 90% of patients with Ménière’s disease no longer experience vertigo and can get on with their normal lives. This technique, widely used in the United States, has been introduced in Spain by Dr Jordi Coromina in the Teknon Medical Centre.
How is vertigo diagnosed?
The first stage of vertigo diagnosis involves the patient answering a series of questions in order to help identify the type of vertigo.
Special attention is paid to how much the vertigo limits day-to-day activity, to evaluate the extent to which the disorder affects the patient and their family.
The second stage of vertigo diagnosis involves a thorough ENT examination, i.e. examination of the ears, nasal cavities, mouth and throat (pharynx and larynx).
The third stage of vertigo diagnosis involves a specialist carrying out the following procedures:
- neurological tests (Images 2, 4, 5, 6 and 7)
- audiometry (hearing tests)
The specialist will perform the following procedures if further examination is needed:
- a specific in-ear balance test called the videonystagmography test (VNG)
- a nuclear magnetic resonance scan (NMR) or a CAT scan (computerised axial tomography) of the ear and brain
The results of the medical history and examinations, together with the hearing and the VNG tests, usually give a clear idea of the location of the vertigo, its cause and, therefore, the appropriate method.
Occasionally, the patient will also be examined by a neurologist who specialises in vertigo.
How is vertigo treated?
Treatment for vertigo varies depending on the symptoms and the type. In the case of Ménière’s disease, treatment is typically as follows:
First, the patient will be prescribed medication only. 70% of patients get better from medication alone, and return to leading a normal life.
If the vertigo does not improve with medication, intratympanic gentamicin treatment is administered. In some cases, an intratympanic injection of cortisone (in the middle ear) will be administered beforehand.
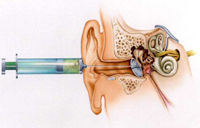
Intratympanic gentamicin injection
Gentamicin is an antibiotic that is used for vertigo or dizziness. It is injected into the eardrum, before travelling into the inner ear and taking effect in the balance mechanism (vestibular system). The gentamicin injection is an outpatient procedure and is performed at our clinic.
The patient should attend weekly check-ups and if improvement is detected, the treatment is stopped. Improvement means a progressive reduction in the intensity, severity and frequency of the episodes of vertigo until they completely disappear. On the other hand, if no improvement is detected, a further injection will be administered (Image. 8).
What can be done if the gentamicin injection does not work
If gentamicin does not work (10% of vertigo cases) a surgical procedure will be performed. Depending on the patient’s hearing, it will be either a vestibular neurectomy or a labyrinthectomy.
The vestibular neurectomy is an incision made to the balancing nerve (vestibulocochlear nerve) in a way that enables the patient to hear.
The labyrinthectomy is the surgical elimination of the internal ear and, consequently, the patient loses residual hearing. This operation is performed in only the most extreme cases in which the condition will eventually override the patient’s hearing.
What treatments exist for other types of vertigo?
The treatment for other variants of vertigo will depend on the underlying cause:
- Benign paroxysmal positional vertigo (BPPV). This form of vertigo is brought on by sudden movements, particularly lying down or sitting up in bed, turning the head from side to side when lying down, overextending the neck to reach something high up, bending down or stooping, etc. These movements irritate the patient’s inner ear and vertigo is brought on due to the misalignment of cells in the inner ear (otoliths), which become stimulated. Treatment involves a repositioning operation, carried out at our clinic, which is aimed at realigning the otoliths. (Images 9 and 10)
- Vestibular neuronitis. This is an inflammatory injury of the vestibular nerve, which causes the patient to experience vertigo or dizziness without internal noise interference or hearing loss. It is a one-off, intense episode lasting 3 to 6 days in which the patient experiences considerable dizziness and nausea, following a sensation of unsteadiness lasting 2 to 3 weeks. The treatment involves performing vestibular rehabilitation exercises.

